
Written by Claire Lowther, Nurse Manager for Coloplast Ltd, and Tracey Murphy senior Coloplast Nurse for Coloplast Ltd. This blog looks at Intermittent self catharisation, what it is and how it can effectively be used to treat patients with retention of urine. We also reflect on a case study of a gentleman who has a spinal cord injury and how choosing the correct product can affect quality of life and potentially reduce Urinary Tract infections (UTIs).
Shackley et al (2017) writing for the British Medical Journal states that the use of urinary catheters is one of the highest treatment options within our healthcare system, with 1 in 5 patients in hospital and 1 in 14 in the community setting being catheterised. The risks of indwelling catheters are well documented and include catheter-associated urinary tract infections (CAUTIs), bacteraemia and increased and urosepsis.
In 2015 the National Institute for Health and Care Excellence (NICE) acknowledged Intermittent selfcatheterisation (ISC) as the gold standard in continence care and this is now the preferred method of bladder management. The reason for this is that not only does ISC put the user in control of their own bladder function and facilitate normal voiding, but it can also reduce the risk of infection and offers greater psychological and physical benefits to a traditional indwelling catheter. (Catheter Care, RCN Guidance, 2019)
What is Intermittent Self Catheterisation?
Intermittent self-catheterisation (ISC) is defined by Shah and Leach (1998, cited in Naish 2003), as ‘passing a catheter into the bladder to remove urine when the patient cannot pass urine normally’. The procedure may be repeated every few hours if necessary and is viewed as an alternative technique to an indwelling catheter as a means of managing urinary problems. ISC is an established intervention (Addison, 2001, cited in Naish 2003) and is recognised as a safe and effective procedure (Moore, 1995, cited in Naish 2003). For many, the thought of undertaking ISC can be daunting, there is for some the fear of undertaking something medical, for others a fear of pain or discomfort. For most patients undertaking ISC, it is an essential task in order to maintain bladder function.

Who can be taught ISC?
Any individual proven to have a significant residual volume of urine over a prolonged period would benefit from ISC. This is because retaining urine is a significant risk factor and cause of urinary tract infections. Patients who undertook ISC would need to have good cognitive function and suitable dexterity or the support of a carer or family member in order to have a successful outcome. It is also important to choose the correct type of catheter to meet their needs, therefore holistic assessment is essential.
Urinary Tract infections (UTIs)
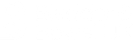
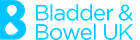
Urinary tract infections are divided into upper or lower UTIs depending on which part of the urinary tract is affected. The urinary tract consists of the kidneys and the ureters, the bladder and the urethra.
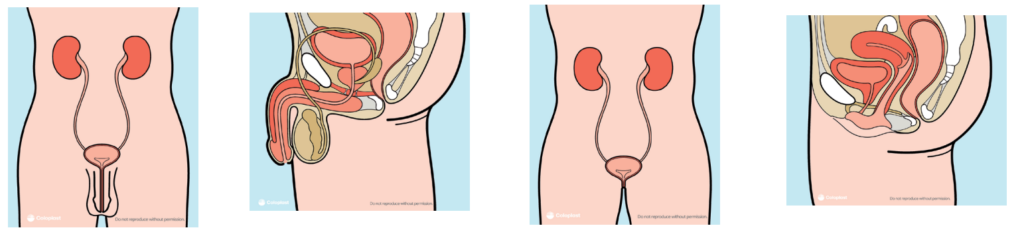
Lower urinary tract infections are much more common than upper UTIs and include the bladder and urethra. Upper UTIs are potentially more serious as they can involve the kidneys. Whilst it might seem a bit daunting that you can get a UTI from using ISC, it is important to remember that the risk of getting a UTI is much higher if you don’t use intermittent self-catheterisation. In fact, one of the key reasons that ISC is often recommended is to reduce the chances of developing a urinary tract infection. However, that does not stop patients worry about them, A Coloplast survey in 2016 of ISC users in the community setting states that 45% of patients worry about getting UTI’s when they self-catheterise. And most expect to get a UTI at least 2-3 times a year which is demonstrated in this case study below.
Case presentation
Bob (pseudonym) is a 62-year-old man with a spinal cord injury. He is paralysed from the neck down and no longer has any natural bladder function. He uses a wheelchair during the day and cannot stand to pass urine. He has chosen to undertake ISC for the last year, instead of having an indwelling catheter, but has experienced several episodes of uro-sepsis and admission to hospital. His wife performs the ISC for him, 5 times a day into a jug.
When we met Bob, he was using a good standard catheter that was functionally adequate however he was keen to explore if there was anything we could suggest that might make his life easier, particularly for his wife, and also help reduce the number of hospital admissions in the future. Owing to recent research we were able to discuss how the friction force of catheters could effect urethral trauma and therefore potentially increase infection rates. By undertaking a detailed consultation and listening to Bob and his wife’s needs we were able to show him a couple of new catheters, one of which has a catheter bag attached and is known as a “set” catheter.
Bob has highlighted to us that he did not go out often – he had never catheterised away from the home, the experience of catheterising usually meant leakage of urine as his wife struggled to catheterise and hold a jug. We were able to show him how to use Speedicath Flex Set, a new catheter that had a bag attached – this bag would capture the urine as ISC is performed, negating the need to use the jug.
Additionally this catheter has a triple action coating technology applied to the catheter – this makes insertion smoother – less friction should mean less trauma to the urethra and therefore long term reduce the potential of urine infections that in the past have led to sepsis.
The detailed consultation also allowed time to explore hygiene aspects with ISC and as the catheter has a sleeve, explain how this reduces the likelihood of cross infection but also discuss with both Bob and his wife the importance of hand hygiene. Bob has been using the catheter for a while now and has not had any further admissions to hospital. Most importantly, Bob has found new freedom. Accompanied by his wife they have managed to get out and about a little. They no longer use a jug and rely on this system to support their needs.
What is Friction Force and Triple action coating?
Within the case study we referred to friction force. A catheter with insufficient hydration can cause friction and irritation to the urethra. On average, catheter users catheterise 5 times a day – which adds up to 1825 times a year, this is why it’s so important that every single insertion and withdrawal of the catheter is as smooth as possible to reduce discomfort and protect the urethra. (Stensballe J et al 2005). The coating on the Speedicath Flex Set catheter that was used in this case study has the triple action coating technology. To protect the mucosa from the risks of damage, complications,** and UTIs,*** it’s important to have a coating that stays bonded, stays smooth and stays hydrated.
All SpeediCath catheters come with a unique hydrophilic coating, featuring our Triple Action Coating
Technology. It consists of three strongly bonded elements, designed to protect the urethra in three ways: it stays bonded, stays smooth, and stays hydrated.
Stays bonded
SpeediCath’s unique hydrophilic coating stays bonded during insertion and
withdrawal due to a proprietary base-coat that is covalently bonded to the catheter
surface for an even coating without dry spots.
Stays smooth
SpeediCath’s unique hydrophilic coating stays smooth because the polymer top-coat
enables excellent water absorption for low friction, smooth insertion and reduced
discomfort compared to uncoated catheters.
Stays hydrated
SpeediCath’s unique hydrophilic coating stays hydrated with a special water-based
solution that swells the coating and makes it instantly ready to use.
Making life easier
It is cases like Bob’s that make us realise how important it is to choose the correct catheter when performing ISC. Using current data, such as friction force data, to help empower patient choice is highly important. ISC offers significant advantages to that of alternative bladder management solutions and when performed well and concordantly will reduce UTIs, improve quality of life and enable independence.
References
1)IC value proposition January 2016: Coloplast survey, CIC users in community setting n=2942 (PM-06287) – on file
- Stensballe J, Looms D, Nielsen PN, et al. Hydrophilic-coated catheters for intermittent catheterisation reduce urethral micro trauma: a prospective,
randomised, participant-blinded, crossover study of three different types of catheters. Sponsored by Coloplast. EurUrol 2005;48(6):978–83, n=49. **
Urethral bleeding (hematuria) and strictures
*** compared to uncoated catheters
• Sharkey et al (2017) Variation in the prevalence of urinary catheters: a profile of National Health Service patients in England. Published in
the British Medical Journal 2017; 7(6): e013842. Found online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5577876/#:~:text=Our%20results%20
indicate%20that%20urinary,more%20prevalent%20in%20males%20overall. (accessed 13th January 2021)
• Vahr S, Cobussen-Boekhorst H, Eikenboom J, Geng V, Holroyd S, Lester M et al (2013) ‘Evidence-based guidelines for best practice in urological health care. Catheterisation; urethral intermittent in adults; dilatation, urethral intermittent in adults’. European Association of Urology Nurses (EAUN).
• Naish, W (2003) Intermittent self-catheterisation for managing urinary problems
• Catheter Care (2019), RCN Guidance For Healthcare Professionals, Pg 33
• https://www.nhsemployers.org/pay-pensions-and-reward/nhs-terms-and-conditions-of-service—agenda-for-change/pay-scales (accessed
10th January 2021)

Comments are closed